‘A penny for the old guy’
Shape without form, shade without colour, Paralysed force, gesture without motion…
Between the idea And the reality Between the motion And the act
Falls the Shadow…Between the conception And the creation Between the emotion And the response
Eliot, T.S. (1925). The Hollow Men.
Falls the Shadow…
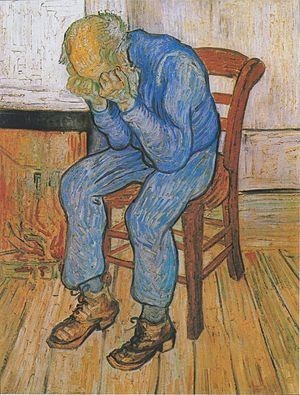
Van Gogh, V. (1890) Sorrowing old man (at eternity’s gate).
..and a glossary to start…
Aboulia: Aboulia or abulia (from Greek: βουλή, meaning “will”,with the prefix –a), in neurology, refers to a lack of will or initiative and can be seen as a disorder of diminished motivation (DDM). Aboulia falls in the middle of the spectrum of diminished motivation, with apathy being less extreme and akinetic mutism being more extreme than aboulia. A patient with aboulia is unable to act or make decisions independently. It may range in severity from subtle to overwhelming. It is also known as Blocq’s disease(which also refers to abasia and astasia-abasia). Aboulia was originally considered to be a disorder of the will.
Anergia: consistently lacking energy or motivation to the point where it is debilitating in everyday life. Sufferers have great difficulty forcing themselves to perform minimal tasks that the typical person would have little to no trouble completing.
Anhedonia: a distinct reduction in the ability to experience pleasure or lack of reactivity to pleasurable stimuli 7.
Asociality: refers to the lack of motivation to engage in social interaction, or a preference for solitary activities. Developmental psychologists use the synonyms nonsocial, unsocial, and social uninterest. Asociality is distinct from but not mutually exclusive to anti-social behaviour, in which the latter implies an active misanthropy or antagonism toward other people or the general social order. A degree of asociality is routinely observed in introverts, while extreme asociality is observed in people with a variety of clinical conditions.
Avolition: is the decrease in the motivation to initiate and perform self-directed purposeful activities. Such activities that appear to be neglected usually include routine activities, including hobbies, going to work and/or school, and most notably, engaging in social activities. A person experiencing avolition may stay at home for long periods of time, rather than seeking out work or peer relations.
‘Double depression’: a “double depression” is the occurrence of episodes of major depression inaddition to dysthymia. Switching between periods of dysthymic moods and periods of hypomanic moods is indicative of cyclothymia, which is a mild variant of bipolar disorder.
Dysthymia: in the DSM-5, dysthymia is replaced by persistent depressive disorder. This new condition includes both chronic major depressive disorder and the previous dysthymic disorder. The reason for this change is that there was no evidence for meaningful differences between these two conditions. The term is from Ancient Greek meaning bad state of mind. Dysthymia is less acute and severe than major depressive disorder. As dysthymia is a chronic disorder, sufferers may experience symptoms for many years before it is diagnosed, if diagnosis occurs at all. As a result, they may believe that depression is a part of their character, so they may not even discuss their symptoms with doctors, family members or friends.
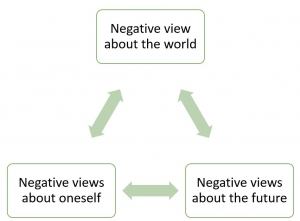
Hopelessness theory of depression…
…with some ‘People’s Poetry’ too …
1. (From ‘Melon Collie and the infinite sadness’ )
And I don’t even care to shake these zipper blues And we don’t know just where our bones will rest To dust I guess
Forgotten and absorbed into the earth below The street heats the urgency of sound
As you can see there’s no one around 2.
2. (From ‘22, A Million’)
Oh the old modus : out to be leading live Said, comes the old ponens *, demit to strive
A word about Gnosis: it ain’t gonna buy the groceries Or middle-out locusts, or weigh to find
I hurry bout shame, and I worry bout a worn path And I wander off, just to come back home Turning to waltz, hold high in the lowlands Cause the days have no numbers
It harms me, it harms me, it harms me- like a lamb 18.
* “Modus ponens”: pretty much means JUMPING TO CONCLUSIONS (but I could be wrong!) Ed.
….and finally, a beginning:
Disclaimer: This self-absorbed rag-tag summary is shared in good will by a layman sufferer and in no way represents the views of Brisbane Counselling Centre…
As a 30+ year sufferer of depression it came as no surprise to me to find that since my heyday, significant advances have occurred in the diagnosis and treatment of the condition, such that an expanded taxonomy of depression now includes (in my opinion, or so I thought) the far more attractive and flattering differential diagnosis of melancholia (ie as opposed to your garden-variety type major or clinical depression).
My interest thus piqued I sought recent articles in the field 3-16. for further information, and, starting as is my want with one of my favourite remaining few trusted aphorisms –a joke always contains 10% of the truth- my pilgrimage began with the urban dictionary:
Melancholia: Basically, it’s a less intense version of depression, though it differs from it in a lot of ways. People who are depressed just feel worthless and think that nothing could cure them or make them happy. However, melancholia isn’t like that and it’s more narcissistic, making the sufferer want ‘better’ feelings (or better life) – longing for love, the past (if nostalgic) and just want their gaps to be filled. They’d daydream about being with what they long for and such.
Ouch! That stings!…but is it right? Well, many bloggers (according to my cursory research) do support such a notion e.g.,
The concept of ‘sadness’ implies grief and a certain hopelessness, while ‘melancholy’ implies a sorrow with purpose, an emotion with which one can be swathed as if it were a shroud….melancholy is comfortable, a lozenge to be masticated for a reason, a sadness that has pensive pleasure melted into it something it’s comfortable to suckle and to be wrapped in.
Hmmm quick cut to ‘the arts’, where melancholia has garnered more interesting press and, to my surprise seems to offer more useful information than most of the ‘scientific’ papers I will refer to below. Firstly is the notion that melancholia strikes the very top levels of one’s existence in a society: it is an epicentric disorder, where even one’s most basic small ‘p’ political beliefs fail to stimulate ANY desire to act.
I cannot but reflect how absent from all my interactions with mental health practitioners has been dialogue even hinting at the following:
…melancholia suggests individual incapacitation, even dissolution, by predatory hangovers from the past…where politics being a communal practice that strives to effect another sense of the world or even create another world, characterised by effects of enthusiasm; melancholia would be a form of individual inaction correlated with a suspension ofany sense of world, and characterized by singular affects of anhedonia and despair.
The very use of the word ‘melancholia’ is therefore meant to take a critical distance from the connotations of the category of depression, which is a term borrowed fromthe economic field and allegedly first used in a technical sense by the Swiss psychiatrist Adolf Meyer in the early twentieth century. 17.
Food for thought there!
Changing tack for yet another perspective, my attention turned to the more romantic, ‘old world’ descriptors I vaguely recalled from my under-graduate years, where melancholia was merely a (if not a little distasteful) ‘normal’ character-set; a manifestation of one of the four ‘humours’, and sympathetically caricatured as ‘the grumpy old man deep in thought’.
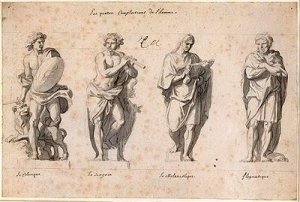
According to Wikipedia, Galen (AD 129 – c. 200) developed the first typology of temperament in his dissertation De temperamentis, and searched for physiological reasons for different behaviors in humans. He classified them as hot/cold and dry/wet taken from the four elements. Galen named “sanguine”, “choleric”, “melancholic” and “phlegmatic” after the bodily humors, respectively. Each was the result of an excess of one of the humors that produced, in turn, the imbalance in paired qualities.
You can find a quiz to determine if you have a melancholic personality type here, which they describe as
..thoughtful, introspective and reserved, melancholics are often the quiet idealists of the bunch. In essence, they crave time alone and are serious, intense and moody, as well as sensitive, perfectionistic and careful in decision making. The Melancholic is the “brooder” of the bunch.
As attractive as this proposition appears to me (what! I’m a malingerer?), I cannot help but think that the pendulum of creditability may have swung too far the other way: time to consult mainstream scientific thought I guess-
Queue the DSM-5 and ICD-10 (and their various iterations)- the handbook/bibles of mental woes- which, surprisingly, according to whose interpretation you trust, also disappoints, displaying as it does a somewhat tenuous grip on the differential diagnosis of melancholia.
…….Enter a champion of the cause, (an Australian) whose ‘several decades’ of work have ‘chipped away’3-5, 11-15 at a longstanding canon of medical treatment- in this case the monolith of depression and its treatment- not motivated, it seems to me, by a desire to prove ‘the authorities’ wrong, but merely seeking to humbly assuage the uneasy feeling (with an inkling that it is shared by others in the field) that:
If melancholia is poorly defined and diagnosed, then estimates of its prevalence, cause, and optimal treatment are compromised 3.
Whistle well and truly blown, I would say. In thus referring readers to the plethora of online and hard copy articles by Dr Gordon Parker, Scientia Professor of Psychiatry, University of New South Wales, I cannot but help myself throwing in some (methinks) apposite quotes and resources to whet the consumer appetite further, namely, his critique of the current guidelines:
DSM-5 criteria for melancholic features and the ICD-10 somatic syndrome criterion share a similar set of symptom criteria (ie anhedonia, non-reactive mood, early morning wakening, depression worse in the morning, psychomotor disturbance, loss of appetite and weight) that capture most of the historically favoured endogeneity symptoms…But.no set of endogeneity symptoms has shown accuracy in differentiating melancholic from non-melancholic depression…,
some fancy MRI data,
…melancholic patients …had decreased connectivity from the insular to the fronto-parietal cortex..When shown emotionally salient films, patients in the melancholic group exhibited decreased functional connectivity in the subgenual anterior cingulate cortex and caudate, which correlated with anhedonia and a non-reactive mood..
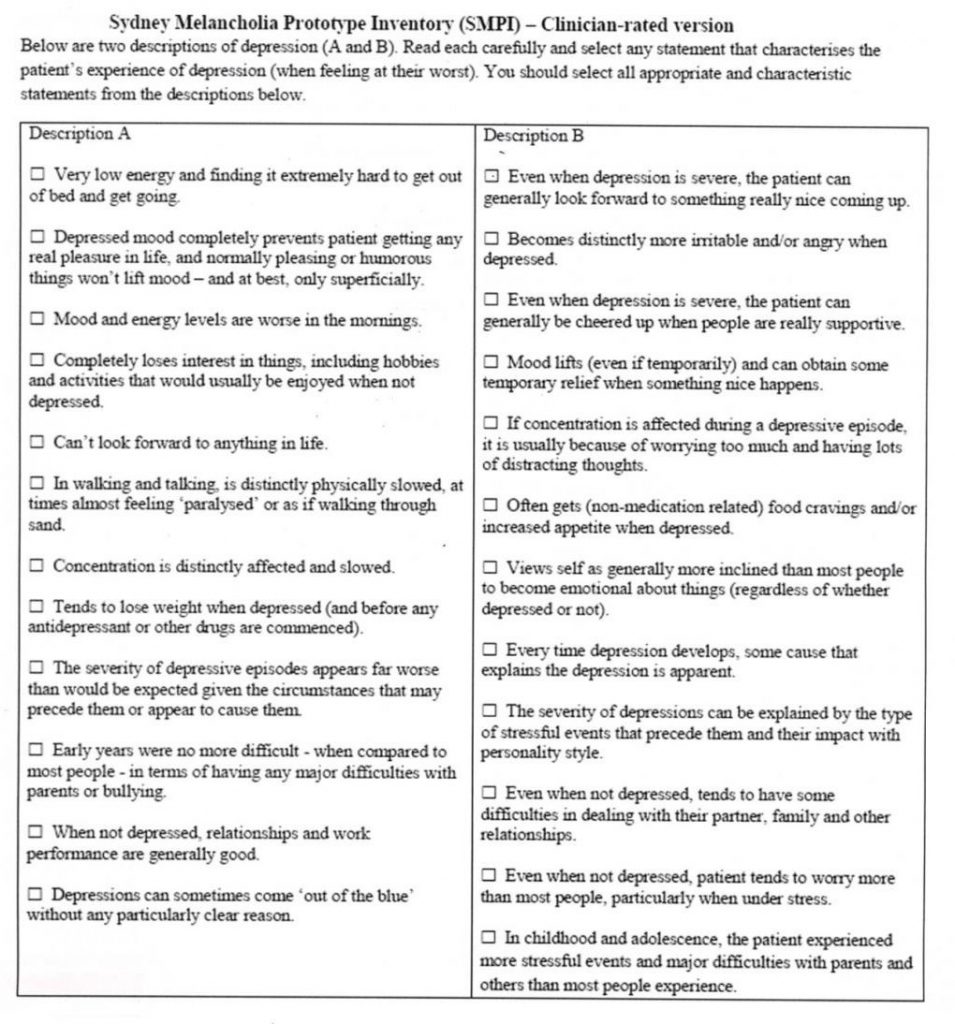
a key diagnostic tool,
(at the risk over overstepping the doctor-consumer boundary) this questionnaire (reproduced for study purposes only from a Dr Parker3. paper), with its take-home message that if one’s scores for each column differ by four or more points, a diagnosis (melancholia vs non-melancholic depression) may be statistically valid:
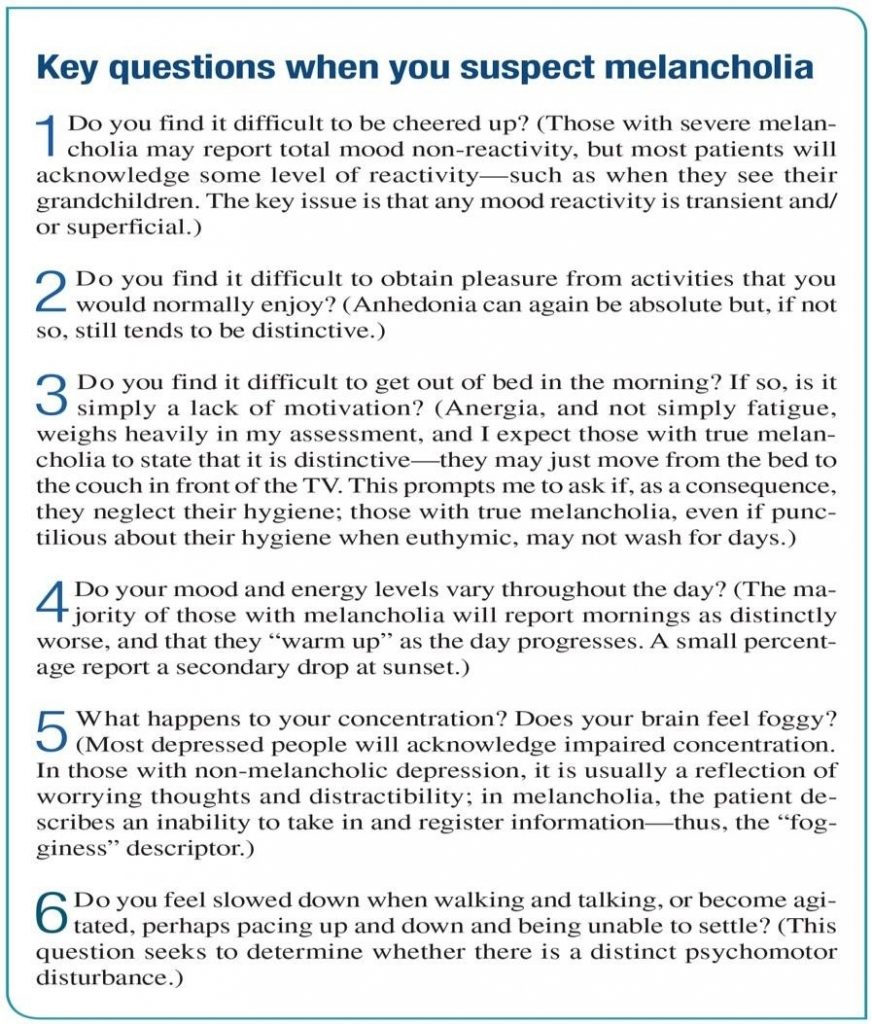
and, the good Professor’s “6 key questions when you suspect melancholia” (again, for study purposes only)…
It works for me- finally (!) my quest has borne some fruit; someone has gotten to the nub. I am relieved, comforted, and feel more supported, confident, and thus motivated to further explore the character of my (lifelong) depression with whosoever is willing to embark on the journey of recovery, be it via conventional psychiatry or the plethora of convergent healers.
Notwithstanding this, for my last take on the subject I can’t but help zoom out from the clinical setting once again, as, whilst I have found psychiatry very helpful in diagnosis and (pharmacological) treatment of my depression, I am still left craving the type of self-understanding that I fear will only come from outside the doctor’s office:
If Freud considered melancholia as a failed mourning – because its triggering loss is unconscious which makes the required work of mourning impossible – our suggestion is to consider melancholia as an antidote to the current understanding of depression as a mere dysfunctionality to be treated by antidepressants. In doing so, we are expressly interested in the world-destroying and world-creating potentials of melancholia – indeed, in a sense, following ‘the loss of the world itself’ that the current situation perhaps presents us with17..
…and, finally, a look to the future, where ‘omics’ (and in particular ‘metabolomics’) is already being touted as a possible solution to the diagnostic quandary. Capitalising on advances in serum/cellular analysis technology (including genomics), the identification of a melancholic ‘footprint’ may not be too far away, enabling widespread testing for ‘the condition’, with a view to increasing the treatment specificity.
Biomarkers can be measured in any biological sample, for example blood, urine, or saliva, and can be indicators of disease traits (or risk markers), disease states, or disease rates (progression),
and
Our extensive experiments on the metabolite data show that strong signals exist in metabolite data that can differentiate melancholic depressive patients from healthy controls 6..
Conclusion
It is now clear that melancholic depression IS real, IS severe, and IS characterised by a validated set of indicators which, at the very least, may be used in dialogue with your mental health practitioner to better manage your particular depression.
References
- Eliott, T.S. (1925) “The Hollow Men”.
- The Smashing Pumpkins (1995); 1979; Mellon Collie and the Infinite
- Parker, (2017). Diagnosing melancholic depression: some personal observations. Australasian Psychiatry, Vol 25(1) 21-24.
- Parker, (2017). Managing melancholic depression: a personal perspective. Australasian Psychiatry, Vol 25(1) 25-27.
- Parker, (2017) An Update on Melancholia. Psychiatric Times, http://www.psychiatrictimes.com.
- Sethi, and Brietzke, E. (2016) Omics-Based Biomarkers: Application of Metaolomics in Neuropsychiatric Disorders. Int J Neuropsychopharmacol, 19 (3).
- Liu, T. et al. (2015). The Hopelessness Theory of Depression: A Quarter Century in Review. Clin Psychol, Dec 1; 22(4): 345-365.
- Fletcher, , Parker, G et al (2015). Anhedonia in melancholic and non-melancholic depressive disorders.Journal of Affective Disorders, 184: 81-88.
- Hyett, P. et al (2015). Disrupted effective connectivity of cortical systems supporting attention and interoception in melancholia. JAMA Psychiatry; 72(4): 350-35
- Thomsen, R. et al (2015). Reconceptualising anhedonia: novel perspectives on balancing the pleasure networks in the human brain. Front Behav Neurosci; 9: 49
- Parker, G. et al (2013). Validation of a new prototypic measure of melancholia. Compr Psychiatry; 54(7): 835-41.
- Parker, G et al (2013). Discriminating melancholic and non-melancholic depression by prototypical clinical features. Journal of Affective Disorders; 144 (3): 199-207
- ‘Crystal’, (2013). Online Forums- Beyondblue. Forums/Depression/Recently diagnosed with Melancholic depression: seeking advice.
- Parker, (2013). A Case for Reprising and Redefining Melancholia. CanJPsychiatry; 58(4): 183-189
- Parker, (2010). Issues for DSM-5: Whither Melancholia? The Case for its Classification as a Distinct Mood Disorder. Am J Psychiatry; 167(7): 745-747
- Day, V., and Williams, L.M. (2012) Finding a biosignature melancholic depression. Expert Rev Neurother; 12(7): 835-47
- Politics and melancholia- crisis and critique (2016). Volume 3/Issue
- Lewis, M.,Vernon,J., and Regan,F. (Bon Iver, 2016). 00000
