
This article expands on The Role of Psychology in Pain Management, focusing on the use of a particular treatment approach: eye movement desensitisation and reprocessing (EMDR).
“Chronic pain is not all about the body, and it’s not all about the brain – it’s everything. Target everything. Take back your life.”
From Stanford’s Sean Mackey, MD, PhD and his lecture “Pain and the Brain”
What is chronic pain (CP)?
Defined as pain lasting more than 3 months, neurobiological research has advanced our view of CP to that of a multifactorial biopsychosocial ‘syndrome’ encompassing genetic, neurological, emotional and cultural factors.
The causes of CP are diverse, from cancer to diabetes to neurological illnesses and other ailments, and includes autogenic (self-generated) pain, where the pain itself becomes the disease.
The majority of CP sufferers have not gone to their pain specialist or GP expecting a referral to a psychologist, and may initially resist and recoil at the idea that a perceived physical problem may involve psychological wellbeing.
Taking into account, however, that the goal of CP treatment is pain management and the improvement of the disability and distress associated with pain (rather than just ‘providing a cure’), the medical mainstream is gradually adjusting to a pain treatment paradigm shift:
In recent years, different studies have observed a strong association between chronic pain and psychological trauma. Therefore, a trauma-focused psychotherapy, such as eye movement desensitisation and reprocessing (EMDR), could be an innovative treatment option(4.)
In the words of eminent EMDR developer and researcher Francine Shapiro:
The goal of EMDR is to not only reduce the negative impact of pain and trauma but also to address the underlying conditions that are often associated with the dysfunctional response to present events.(12.)
The symptoms and effects of long-term pain
According to a recent study(6.), chronic pain significantly impairs the physical, social, psychological, and financial well-being of those who suffer daily, on both an individual level and a social level. Chronic pain has become a vast social burden that extends well beyond the individual who suffers.
Chronic pain is known to increase psychological disorders, predominantly anxiety and depression, and to decrease the quality of life for both those suffering from chronic pain and for those who are charged with caring for those with chronic pain. Other common difficulties include struggles performing everyday activities, such as engaging in physical exercise, sleeping, walking, completing domestic chores, participating in social events, and being independent.
Isolation also causes a collective loss since those who suffer are often significantly constricted regarding what they can do outside of their homes. Indeed, CP permeates all aspects of a person’s life, and can lead to(2.):
- substance misuse
- social withdrawal and isolation
- depression/anxiety
- heightened stress response
- relationship problems
- decreased libido
- sleep difficulties
- concentration and memory difficulties
- avoidance behaviour
- adverse experiences to medications
- proneness to sudden outbursts of anger
- weight gain
- feelings of negative self-worth
Chronic pain and trauma: the neural network overlap
In the 1980s, pain researchers discovered the phenomenon of ‘central sensitisation’: after repeated painful stimuli, centralised pain transmission neurons attain a state of heightened sensitivity, whereby a subsequent seemingly innocuous stimulus (eg the slightest touch around a cut) causes a pain response. Indeed, the ‘somato-sensory’ system can remain hypersensitised long after an injury has healed, become hypersensitised due to other maladies (neuropathic pain- fibromyalgia, irritable bowel syndrome etc) or nociceptor (specialised pain neurons) damage (chemotherapy, diabetes etc), and even enter a ‘top-down’ hyperarousal state via brain centers regulating thoughts and emotions.
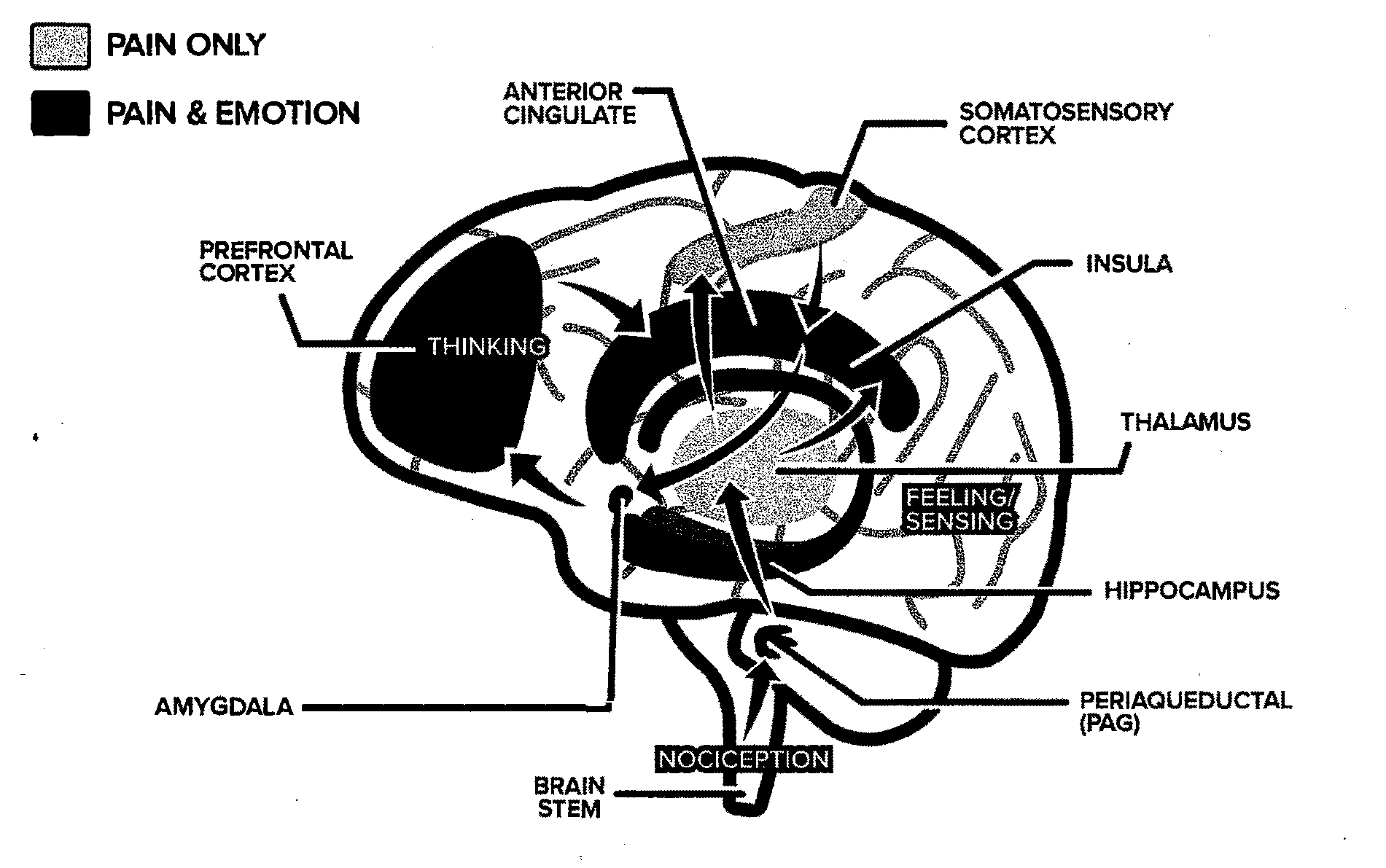
There is no single pain center in the brain..multiple regions are involved including those involved in emotion, cognition, memory, and decision-making.(1.)
In the evolution of psychotherapeutic approaches to CP management, neurobiological research (including deep brain stimulation (DBS) and the use of virtual reality technology) has added credence to intuition-based innovation, with pain and trauma clearly analogous on many levels.
Between 10% and 50% of patients receiving tertiary care treatment for chronic pain have symptoms indicative of psychological trauma and posttraumatic stress disorder(5.). Moreover, chronic pain is associated with higher exposure to psychological trauma.
Pain-trauma pathways and neuroanatomy
If your body is screaming in pain, whether the pain is muscular contractions, anxiety, depression, asthma or arthritis, a first step in releasing the pain may be making the connection between your body pain and the cause. Beliefs are physical. A thought held long enough and repeated enough becomes a belief. The belief then becomes biology.
Marilyn Van M. Derbur,(2003) Miss America by Day
Co-existing with the autonomic nervous system (including ‘stress hormone’ regulation), the body’s response to pain and stress overlap in the brain’s ‘Default Mode Network’ which is responsible for many internal thought processes aimed at helping us survive including decision-making, attention, memory, and task management. Here the sensory, emotional, and cognitive (attention, memory, and thinking) components of pain and stress are resolved to produce a focused response.
As described in a previous article, the principle mechanisms of action of EMDR involve the structures above and similarities abound between CP and post traumatic stress disorder including elevated emotional distress, increased emotional lability, avoidance, hyperarousal and hypervigilance. Furthermore physiological, affective, and behavioral components of pain and trauma are co-reinforcing.
Existing treatments vs EMDR: the research evidence
Despite extensive research, traditional psychological treatments of chronic pain (cognitive behavioural therapy (CBT), acceptance commitment therapy (ACT), mindfulness, biofeedback, hypnosis) suffer from high drop-out rates, weak treatment effects and weak retention of treatment effects(6.).
A recent review(7.) of 26 peer-reviewed studies of EMDR treatment of pain dating from the early 2000’s concluded:
Patients in the EMDR treatment groups showed significantly reduced pain intensity and improved quality of life and anxiety and depressive symptoms compared to ‘treatment as usual’. Post-treatment. improvements were largely maintained at 3-month follow-up. This study suggests that EMDR may be an effective and safe psychological intervention to be used within the multidisciplinary treatment plan of patients with CP.
Importantly,
there is preliminary evidence for the efficacy of EMDR in both chronic pain and acute pain. These results suggest that it is not so much the original origin of the pain that is important for the treatment response as the association of pain symptoms with stressful memories, thoughts, or feelings(9.).
How EMDR works in pain treatment
General EMDR treatment utilises a comprehensive eight-phase protocol that addresses past, present, and future contributors to current psychological disturbances. During EMDR, the patient concentrates on a negative traumatic memory, body sensation, or pain while also focusing on an external bilateral stimulus, (eye movements, sound or tapping/vibration). EMDR is guided by the ‘adaptive information processing’ model (AIP) that views distressing or traumatic memories that are stored in the brain as giving rise to maladaptive thoughts, emotions, sensations, or behaviors unless the information contained in the memories has been adequately reconsolidated(8.).
The AIP model is also consistent with the kindling/central sensitisation model of chronic pain which posits that repeated exposure to painful stimuli leads to increased sensitivity to later noxious stimuli. Operationally, EMDR therapy also works differently to traditional approaches. For example, one of the key change processes in EMDR is accessing internal positive memory networks, as opposed to externally providing “corrective information”.
Whilst many studies support the effectiveness of the ‘standard’ EMDR protocol to focus on the processing of traumatic memories associated with pain, newer research suggests that the pain itself can be targeted and processed by using modified “pain-specific” protocols. In such protocols, special attention is often paid to
- the option of targeting the pain (as opposed to a memory)
- the processing of pain-associated fears
- enabling changes in pain sensations
- developing new coping strategies based on the above changes
- exploration of themes of control, responsibility, and self-image
Finally, it should be noted that EMDR is an ‘integrative’ tool; that is, it may be used in conjunction with other psychological treatment strategies- a qualified (EMDR Association of Australia-certified) and experienced psychologist is recommended for guidance in treatment planning(10.).
If you feel that you would benefit from EMDR in your pain treatment, please feel free to contact us.
References:
1. Bhattacharjee, Y. (2020). A World of Pain. National Geographic, Jan 2020 Wellness Issue. Pp 47-70.
2. Stewart, D. (2021) Working with Clients Experiencing Injury and Pain. Inpsych Feb/Mar 2021. Australian Psychological Society.
3. Grant, M.D.(2014). Eye movement desensitization and reprocessing treatment of chronic pain. OA Musculoskeletal Medicine 2014 Aug 17;2(2):17.
4. Suárez, N.A. (2020). EMDR Versus Treatment-as-Usual in Patients With Chronic Non-Malignant Pain: A Randomized Controlled Pilot Study. Journal of EMDR Practice and Research, Volume 14, Number 4, 2020.
5. Tesarz, J et al.(2013). Effects of eye movement desensitization and reprocessing (EMDR) on non-specific chronic back pain: a randomized controlled trial with additional exploration of the underlying mechanisms BMC Musculoskeletal Disorders 2013, 14:256 http://www.biomedcentral.com/1471-2474/14/256
6. Von Baeyer, K. (2020). Eye Movement Desensitisation Reprocessing (EMDR) as a Treatment For Chronic Pain. ProQuest LLC, Ann Arbor, MI 48106 – 1346.
7. Scelles, C., Bulnes, L. (2021). EMDR as Treatment Option for Conditions Other Than PTSD: A Systematic Review . Front. Psychol. 12:644369. doi: 10.3389/fpsyg.2021.644369
8. Marcus, S.V. (2008) Phase 1 of Integrated EMDR- An Abortive Treatment for Migraine Headaches. Journal of EMDR Practice and Research, Volume 2, Number 1, 2008 15
9. Tesarz, J et al. (2019). EMDR Therapy’s Efficacy in the Treatment of Pain. Journal of EMDR Practice and Research, Volume 13, Number 4, 2019
10. Tew, M. (2022). Are you sure about using EMDR with pain? Exploring the latest evidence. (March 2022) — EMDR Solutions. https://www.emdrgateway.com/news
11. Grant, M. (2020). Change Your Brain Change Your Pain. www.overcomingpain.com. ISBN: 978-1-925457-24-7
12. Shapiro, F., & Laliotis, D. (2011). EMDR and the adaptive information processing model: Integrative treatment and case conceptualization. Clinical Social Work Journal, 39(2), 191–200.
13. Yam, M.F. et al. (2018). General Pathways of Pain Sensation and the Major Neurotransmitters Involved in Pain Regulation. Int J Mol Sci. 2018 Aug; 19(8): 2164.
