Unswayed by the popular media frenzy surrounding it, this article aims to describe the fundamentals and utility of Porges’(1.) Polyvagal Theory in enhancing modern evidence-based psychotherapy.
Introduction: a psychophysiological research-based theory
To be clear, ‘Polyvagal theory’ (PT) was not developed as a stand-alone therapy, but rather achieved recognition as a possible enhancement to, or platform on which to rest, relevant psychotherapeutic approaches- particularly trauma-related treatments, which had already been seen to benefit from neurobiological imaging and psychophysiological research-based modelling co-opted by prominent therapists including Bessel van der Kolk, Peter A. Levine, Marianne Bentzen, and Dan Siegel.
Notwithstanding the lack of available randomised controlled trial findings (the gold standard of comparative psychotherapeutic outcomes research) to date, trained proponents of approaches which have integrated the theory to a demonstrative degree of success have gone so far as to exhort a ‘polyvagal-informed’ generic qualifier when touting their particular skillsets.

A historical context- the polyvagal leap
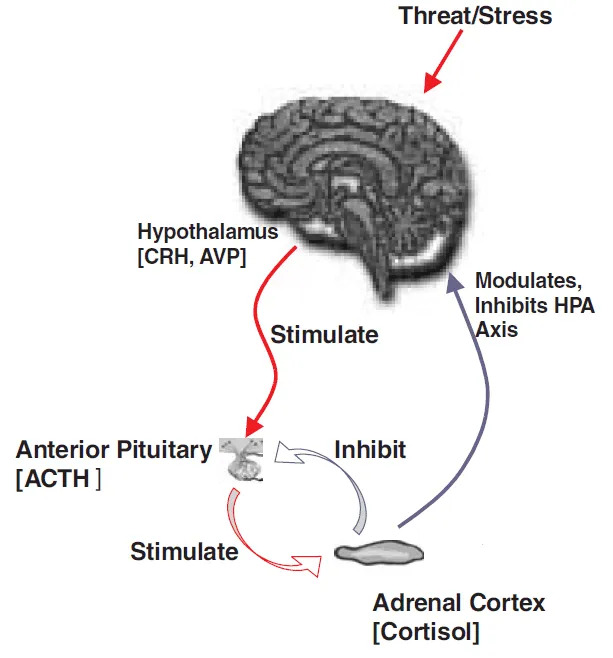
Emerging from arousal theory in the 1960s, and abetted by a shift in focus toward the role of a major nerve-hormone pathway (the HPA) in linking the autonomic nervous system (ANS) to stress-response (‘fight or flight’) behaviour, was the Neurovisceral Integration Model still taught in schools and universities today.
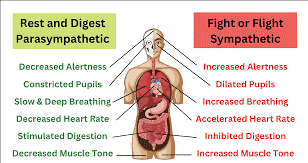
From this linear sympathetic-centric view, researchers were led in earnest toward hypotheses which might explain the famous ‘vagal paradox’(2.)(the vagus can be beneficial and harmful) and thus began targeting the role of the parasympathetic (vagal) branch of the ANS in dampening the impact of the sympathetic-adrenal reactions observed to affect threat response cognition/behaviour.
The 1970s witnessed an explosion of interest in the vagus nerve (an interest that continues to this day in some fields), spawning much discussion regarding ‘the vagal brake’ and popularist claims that vagal stimulation exercises may benefit mental health and wellbeing. Drowning out the ‘we told you so’ alternative medicine choristers, ‘ways to boost your vagus’ (without surgery) became all the rage.
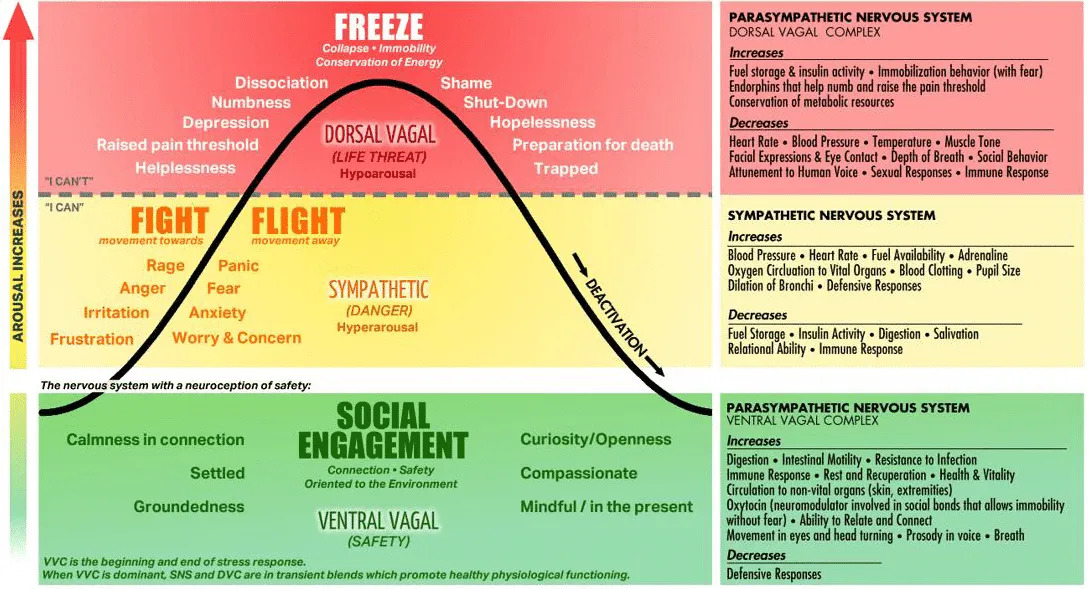
Then in the early 90s, critically, Porges’ PT proposed that the two separate vagal pathways belonging to the parasympathetic nervous system (a dorsal vagal complex (DVC) and a ventral vagal complex (VVC)) contribute to distinctly different biobehavioural roles, constituting a tri-‘state’ model of (now) ‘fight/flight/freeze’ behaviour (..stay tuned for ‘fight/flight/freeze/fawn/fib’):
| ANS Pathway | ‘State’ | Worldview and Associated Emotions |
| Ventral vagal complex (VVC) | Ventral vagal | A state of safety, connection, social engagement: confident, eager, hopeful, compassionate, grounded |
| Sympathetic nervous system (SNS) | Sympathetic | A protective flight-or-flight response, danger cues- Movement, mobilisation: overwhelmed, irritated, stressed |
| Dorsal vagal complex (DVC) | Dorsal vagal | A protective response of freeze, shutdown, dissociation: disconnected, hopeless, low energy, foggy, ashamed |
Polyvagal theory offers a comprehensive perspective on the ANS and its role in shaping human responses to stress, social interactions, and emotional regulation.
Indeed, seen by many to ‘fill the gaps’ intuited from clinical experiences disconsonant with traditional ANS theory, it may be argued that, viewed through the ‘polyvagal lens’, we:
1. recognise ourselves as social animals– Porges’ assertion that the VVC modulates a ‘social engagement system (SES)’, whereas the DVC primarily works with the sympathetic system to preserve homeostasis by adaptively responding to threats, and,
2. are finally ‘allowed’ to react to the same stressor differently to the person next to us and indeed differently to ourselves at different times- Porges’ proposal ‘that autonomic state functions as an intervening variable mediating the response’(2.).
How is polyvagal theory ‘informing’ psychotherapy?
In a nutshell, after reiterating that our early experiences primarily shape our ANS, PT asserts that on-going internal and inter-personal experiences move us through a continual cycle of mobilisation, disconnection, and social engagement (corresponding to sympathetic, DVC, and VVC ‘states’ respectively) as we respond to our changing environment(3.).
These ‘polyvagal states’ are commonly represented graphically and utilise thematic metaphors to illustrate the hierarchy principle (see below)-

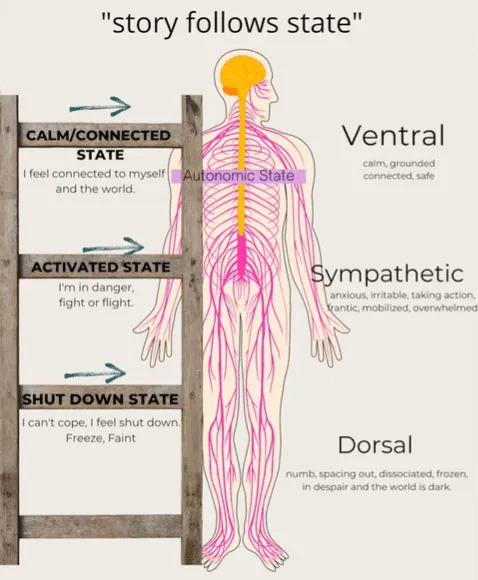

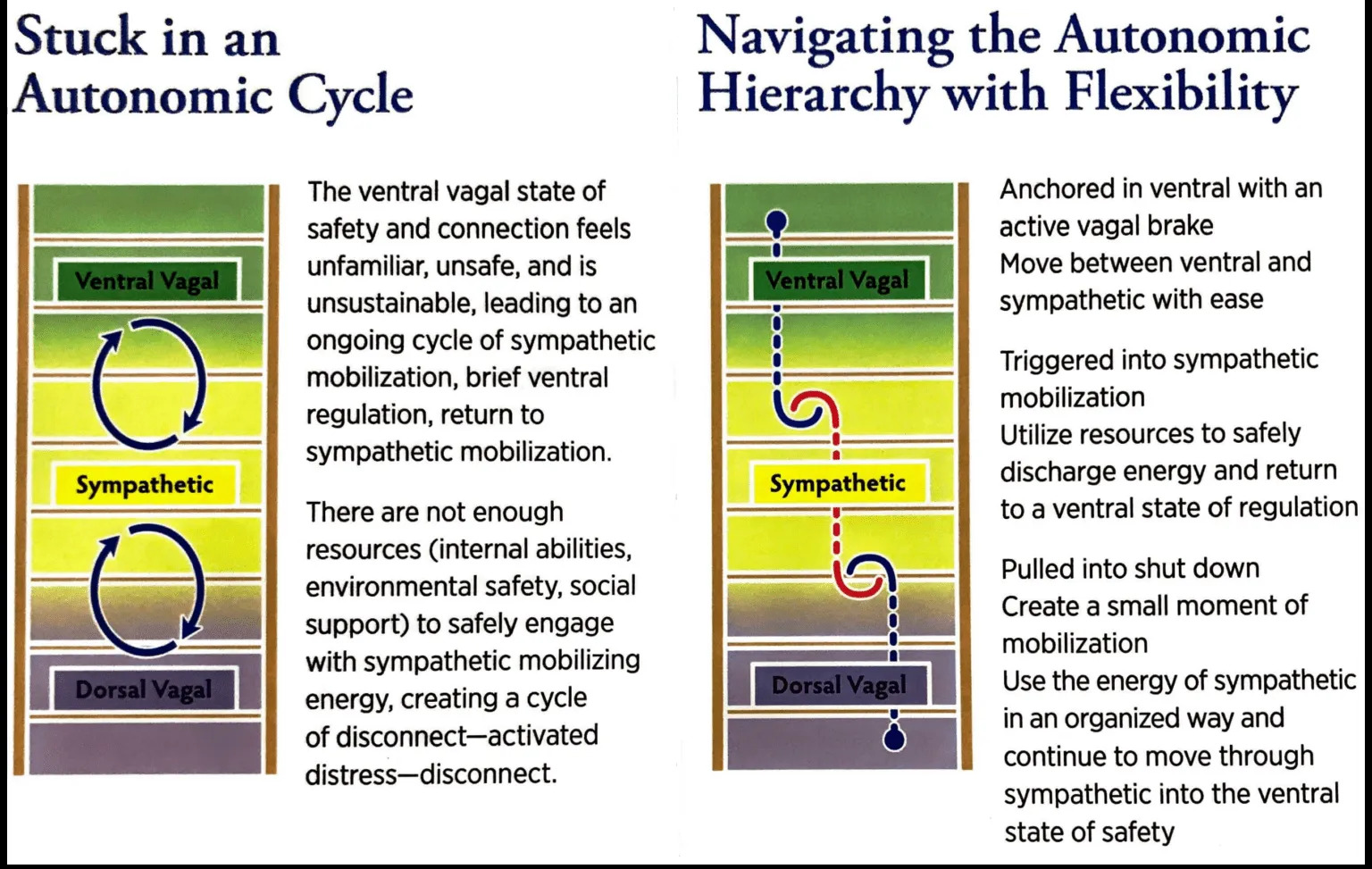
…or diagrams..
– derived from the ‘official’ Polyvagal Association schematic:
Its utility arises from its application as a guide to modifying the ANS in order to facilitate movement away from habitual patterns of fight, flight, and collapse toward connection with self and others.
In essence, this movement is facilitated in a psychotherapeutic context by neural training delivered by a ‘polyvagal-informed’ therapist(4.).
According to PT, it is possible to strengthen a nervous system that has been dysregulated. Repeated exercises inducing oscillation between states, or, steps up or down the ladder (i.e. ‘pendulum exercises’) are purported to ‘condition’ the nervous system, widening ‘the window of tolerance’ such that the ability to rapidly re-regulate is achieved and engrained.
Breath work, mindfulness, yoga, and embodiment exercises (including ‘body scanning’, and interoception tasks) may be utilised.
Additionally, PT-informed therapy alludes to a re-invigorated understanding of our sense of self:
This psychophysiological perspective emphasizes the foundational function of autonomic state in the subjective experiences of global feelings and specific emotions. Within this hierarchical conceptualization, feelings of safety are preeminent and form the core of an enduring motivational system that shifts autonomic state, which in turn drives behaviors, emotions, and thoughts. The resulting model suggests that feelings of safety reflect the foundational autonomic state supporting maturation, health, and sociality(12.).
The guiding principles of PT
The principle of hierarchy
In Porges’(2.) words:
The model can be conceptualized as a stimulus-organism-response model in which autonomic state is expressed and experienced along a continuum from fear-related immobilization involving dorsal vagal mechanisms, to fight-flight mobilization involving sympathetic mechanisms, and finally to a calm socially accessible state involving ventral vagal mechanisms.
Through Porges’ hotly-contested use of the premise ontogengy recapitulates phylogeny (regarding myelination within the brainstem(1.-2.)) he expounds on the particulars of movement within this continuum:
This sequence is hierarchical, with the latter state functionally having the capacity to co-opt the other states to enable hybrid states of mobilization without fear (play, dance) and immobilization without fear (shared moments of intimacy).
The principle of ‘neuroception’
Porges coined this term to describe the way our autonomic nervous system scans for cues of safety, danger, and life threat without involving the thinking (conscious) parts of our brain (i.e. our ‘perceptions’).
From a neuroception of unsafety, there is a move toward sympathetic mobilization or dorsal vagal collapse.
Similarly when safe, the VVC kicks in- safety cues lead to the inhibition of survival responses so that we can socially engage(4.).
A third researcher states:
..neuroception is carried out through a neural reflexive process that is able to immediately shift physiological state and to distinguish visceral and environmental characteristics that are safe, dangerous, or life-threatening.
When environments are safe, a neuroception of safety favors the SES, and the SNS activation is adaptively dampened to preserve the central nervous system that is highly oxygen-dependent, in particular the cortex, from the activities of the DVC (e.g., fainting) that are highly metabolically conservative.
In contrast, a neuroception of danger, or life threat, favors activation of the SNS or DVC, respectively. The organization of these specific circuits, along with the SNS, can influence the individual experiences of body awareness by modulating information that emerges from the body through top-down post-processing, including cortical areas informed by the signals traveling through the body-integrative circuits of the brain(4.).
The principle of co-regulation
PT proposes that through our connection to others (particularly in infancy) and the reciprocal regulation of our ANS, we can move into safe relationships: co-regulation grounds us in a sense of safety and belonging.
The SES encompasses the neural substrates of a range of behaviours and physiological states related to social interaction, communication, attachment, bonding, and interpersonal connections.
The social engagement system involves our ears, eyes, voice, and head via the VVC and connections to the heart and brain. SES is a scanning system that searches for cues of safety, and signals safety ––‘you can come closer’(4.).
To put it another way, the neural detection of environmental risk establishes the preferential activation of the SES, or the subsequent hierarchical progressive recruitment of the SNS or the DVC(5-6.).
In addition, the anatomical structures involved in the social engagement system have neurophysiological interactions with HPA neuropeptides (including oxytocin), and the immune system. Thus, the SES provides a theoretical model to explain the interactive and stress-related functions of several physiological systems that have central regulatory components, but are expressed in the periphery.
Two take-home’s regarding co-regulation and the SES:
1. We need co regulation (connection) to feel safe. One person’s physiology is regulated in connection (mirroring, mimicking) with another’s. Many of us have experienced this ’emotional contagion’: e.g. feeling tense when someone else is.
2. We need to learn to co regulate not only to survive, but to be able to learn to adequately self regulate, otherwise, it is likely we’ll adopt maladaptive self-regulating behaviours including the use of substances or behaviours to force a change of (mood) state.
What’s all the fuss about polyvagal theory?
The first wave: This fuss, it turns out, is mainly academic, as an explosion of independent research has challenged Porges’ ‘three-part’ ANS model on the basis of its neurophysiological and neuroevolutionary premises.
For those interested, I reference but one(7.) of many respected journal papers which validate his work, and recommend Porges’ own 2023 paper(3.) addressing contended aspects of the theory.
The after-shock: This fuss is yet to fully develop as PT is embraced by an ever-widening circle of ‘polyvagal-informed’ influencers in fields including education, parenting, corporate and government HR management, life coaching, and victim advocacy- just to name a few.
Some examples:
| That’s what we’re trying to do in schools. Students and staff need to know what their nervous systems need when they become dysregulated. This starts with being able to name their ANS states and then know how to access interactive resources from inside themselves, outside in the environment, and between others in relationships(8.). |
| We propose replacing Stockholm syndrome with ‘appeasement,’ a term that can be explained through a biopsychological model (i.e. Polyvagal Theory) to describe how survivors may appear emotionally connected with their perpetrators to effectively adapt to life-threatening situations by calming the perpetrator(9.). |
| Using polyvagal theory as a theoretical framework provides a clear rationale for the present study in investigating the neurobiological mechanisms of individuals with anxious attachment who engage in IPS (Intimate Partner Stalking)(10.). |
| Within the legal system, there’s been a lot of issues when a person hasn’t fought of a predator. And I think this is being poorly informed about how bodies respond(11.). |

Why might I be interested in PT within a psychotherapeutic context?
People are not moved by events but by their interpretations.
Epictetus, Stoic, acknowledged by founder Albert Ellis for inspiring the development of Rational Emotive and Cognitive Behaviour Therapies.
1. Put simply, it may provide a ‘better intuitive fit’ for some people (a more plausible explanation of their social, emotional and communication experiences) than that achieved by applying other theories.
…there may be a range of reactions among individuals who share the same environmental context, but who are in different autonomic states.(12.)
In particular, PT acknowledges the role of the autonomic nervous system in trauma reactivity. Indeed, the internet is replete with (so far largely ‘unofficial’) protocols integrating PT with trauma-focused interventions, such as Trauma-Focused Cognitive Behavioural Therapy (TF-CBT) and exposure therapies including Eye Movement Desensitization and Reprocessing (EMDR).
2. Similar to other integrative (neurobiologically-based) theories (e.g. the ‘window of tolerance’) PT provides a new (and arguably more refined and de-stigmatising) framework for understanding how dysregulation leads to unhealthy behaviour patterns.
When we are autonomically dysregulated and experience a survival response, turning toward a resource that brings the possibility of relief can induce powerful impulses.
Whilst acting on impulse might fail or be maladaptive (unhealthy in the long-term) it is an authentic attempt to resolve the pain of the present whole-of-state experiences; in other words, an attempt at self-regulation.
Food, substances, and “feel-good” behaviours such as gambling and sex are common examples of resources that many people utilise (and may eventually want to change their relationship with).
Understanding the autonomic need to ensure survival, people can be helped to see their ‘resource responses’ without shame(13.).
3. A clearer understanding of Mindfulness based approaches.
According to PT, mindfulness-related and compassion-related meditations would represent neural exercises broadening the ability of the VVC to govern the current state and to favor resilience. In addition, mindfulness-related and compassion-related meditations comprise a range of practices whose aim is to accomplish a similar efficacy in improving autonomic regulation, providing greater psychological and physiological flexibility and tolerance by leveraging emotional reactivity and ameliorating the physiological reactivity threshold(5.).
4. A safer (and therefore stronger) therapeutic alliance.
Ancilliary to 1-3 above, and of particular relevance to individuals with trauma-dysregulated ANSs where physiological reactivity thresholds may be already altered, the context in which a treatment is delivered becomes important, because the treatment process itself can trigger cues in the nervous system which may (to use extremes) render it either defensive/resistant or available/amenable to treatment.
A PT-informed approach emphasises in-the-moment awareness of ANS state and incorporates an understanding of the dynamics of danger/safety cues in the therapeutic setting. Attunement, co-regulation, and the therapist’s regulation of their own autonomic state can promote safety and trust, and thus strengthen the therapeutic alliance (a dominant linear correlate of therapeutic efficacy).
Additionally, psychological incongruence (e.g. smiling when talking about something sad) and dissociation/detachment effects are accommodated by PT-informed approaches, and anger ‘re-read’ as an efficient guide and tool in shifting between states.
From one prominent therapist(4.):
Our ANS has expectations and when they are violated, we can experience neuroception of danger.
…when a person has experienced closeness and openness with another as dangerous, and the therapist responds with calmness and validation, this is also a violation, but a positive one, that interrupts neuroceptive expectations.
From a Polyvagal viewpoint, these discomfirmations are small, but essential steps in the healing process.

What about the criticisms of PT?
A reliable analysis of criticism being beyond the scope of this article (the many challenges and rebuttals are widely available online), a ‘buyer beware’ attitude may be advisable despite Porges’ reassurance that virtually all of the over 14 000 peer reviewed foundational articles explaining and expanding PT theory cited on Google Scholar up to Dec 2022 are supportive of the theory(3.).
Regarding its application, recent assertions and counterarguments include:
A worrying trend in the upcoming world of therapy based on the Polyvagal Theory is the emphasis on the superiority of the ventral vagal states.
..(from one researcher)..’we are not proposing that the only final goal is the cultivation of VVC, the theoretical association with the neural substrate of the VVC may be viewed as a neurophysiological platform for the advent of states such as social connection. Analogously, we do not wish to propose that the neural platforms other than VVC are “bad”, as these neurophysiological states are adaptive in comprehending the complexity of human behavior and experience‘..
(PT) is all good and well -maybe?- in a normal population, but what happens when we start working with people who often live and breathe the dorsal states? Like people on the autism spectrum?
..clearly based on circular reasoning, a nonetheless cautiously unqualified(16.) reply might be: pending more targeted research, specialist advice should be sought before applying the approach in cases where ‘neurodivergence’ may be a confounding variable.
Conclusion
Written for educational purposes only, the material in this article in no way represents the views of Brisbane Counselling Centre. Notwithstanding this you are welcome to contact the Centre for further information if you are interested in accessing the services of a ‘polyvagal-informed’ practitioner.
References
1. Porges, S.W. (1995). Orienting in a defensive world: Mammalian modifications of our evolutionary heritage. A Polyvagal Theory. Psychophysiology, 32 (1995), 301-318.
2. Porges, S.W. (2001). The polyvagal theory: phylogenetic substrates of a social nervous system. International Journal of Psychophysiology 42, 123-146..
3. Porges, S.W. (2023). Polyvagal Theory: Summary, Premises & Current Status. Polyvagal Institute Inc.
4. Dana, D. (2018).The Polyvagal Theory in Therapy. Engaging the Rhythm of Regulation . New York, NY: W.H.Norton & Company.
5. Poli, A., et al. (2021). A Systematic Review of a Polyvagal Perspective on Embodied Contemplative Practices as Promoters of Cardiorespiratory Coupling and Traumatic Stress Recovery for PTSD and OCD: Research Methodologies and State of the Art. Int. J. Environ. Res. Public Health 2021, 18, 11778.
6. Kolacz, J., Porges, S.W., et al. (2019). Traumatic stress and the autonomic brain‐gut connection in development: Polyvagal Theory as an integrative framework for psychosocial and gastrointestinal pathology. Developmental Psychobiology. 2019;1–14.
7. Taylor, E.W., et al. (2022). An overview of the phylogeny of cardiorespiratory control in vertebrates with some reflections on the ‘Polyvagal Theory’. Biological Psychology 172.
8. McCraty, R.; Zayas, M.A. (2014). Cardiac Coherence, Self-Regulation, Autonomic Stability, and Psychosocial Well-Being. Front. Psychol. 2014, 5, 1090.
9. Bailey, R. et al. (2023). Appeasement: replacing Stockholm syndrome as a definition of a survival Strategy. European Journal of Psychotraumatology VOL. 14, NO. 1, 2161038.
10. Stellar, J.E.; Cohen, A.; Oveis, C.; Keltner, D. (2015). Affective and Physiological Responses to the Suffering of Others: Compassion and Vagal Activity. J. Pers. Soc. Psychol. 2015, 108, 572–585.
11. Bailey, R., & Bailey, E. (2022). Effective communication with participants in court hearings: using polyvagal theory in the courtroom. Juvenile and Family Court Journal. 73. 57-66.
12. Porges, S.W. (2022). Polyvagal Theory: A Science of Safety. Front. Integr. Neurosci. 16:871227.
13. Porges, S.W., Dana, D. (Eds.). (2018). Clinical applications of the polyvagal theory: The emergence of polyvagal-informed therapies. W. W. Norton & Company.
14. Simon, D.; Adler, N.; Kaufmann, C.; Kathmann, N. (2014). Amygdala Hyperactivation during Symptom Provocation in Obsessive–Compulsive Disorder and Its Modulation by Distraction. NeuroImage Clin. 2014, 4, 549–557.
15. Scaer, R. (2014). The body bears the burden: Trauma, dissociation, and disease. Routledge.
16. Bridges, H. (2015). Reframe Your Thinking Around Autism: How the Polyvagal Theory and Brain Plasticity Help Us Make Sense of Autism. Jessica Kingsley Publishers.
