
This article aims to address issues of individual and family access to psychologists for National Disability Insurance Scheme (NDIS) participants and prospective entrants. Whilst all care has been taken in the fact-based rendering of opinion expressed here, readers are reminded that the National Disability Insurance Agency (NDIA) is ultimately responsible for interpreting and administering the NDIS Act (Cth, 2013) and its amendments.
..impairment does not derogate human dignity nor does it encroach upon the disabled person’s status as a rights bearer.
Theresia Degener, Laws (2016) 5, 35, p.8.
From ‘the rolling quads(1.)’ to ‘download Access Request Form’: a brief history of the NDIS.

Described as the most significant social service reform in Australia since Medicare(2.), and, building on The Disability Services (Cth,1986) and Disability Discrimination (Cth, 1992) Acts, the NDIS arguably achieves a gestalt of 1960s disruptive activism and peri-millennial neoliberal ‘passive revolution’, with residual discourse now predominantly aimed at ‘fine-tuning’ the nascent brainchild of the consumer sovereignty-touting Productivity Commission and the NDIA.
Notably(3.), the first objective of The Act is to ‘give effect to Australia’s obligations under the 2006 United Nations’ Convention on the Rights of Persons with Disabilities.
Between 2016 and 2022, a laudable degree of collaboration produced several legislative amendments including provisions strengthening worker screening, governance, supports for ‘at risk’ participants, and service delivery standards, whilst, in a demonstration of consistent fidelity to a consultative ethos, at least one proposed amendment (independent assessment provisions(4.)) was respectfully abandoned during the period due to sound opposing arguments.
Viewed through the disability activism lens however, mental health, first brought into focus by chilling public stories exposing abuse and violence of people with disabilities within large psychiatric institutions during the latter 20th century(1.), was accommodated tardily.
No. He isn’t extraordinary. He is simply a man and no more, and is subject to all the fears and all the cowardices and the timidity that any other man is subject to. Given a few more days, I have a very strong feeling that he will prove this, to us as well as the rest of the patients.
Nurse Ratched, from One Flew Over the Cuckoo’s Nest, Kesey, K. (1962). USA, Viking Press.
Indeed, whilst the marketised service ‘consumer’ terminology adopted by the NDIS first appeared in the 1992 National Mental Health Policy, the NDIA did not establish a psychosocial stream for the NDIS (via engaging Mental Health Australia to run consultations in relation to a design pathway) until 2018(5.).
Mental Health and the NDIS: psychococial disability
Psychosocial disability is the term used to describe disabilities that may arise from mental health conditions. Whilst not everyone who has a mental health issue will experience psychosocial disability, those that do can experience severe effects and social disadvantage. People with a significant disability that is likely to be permanent may qualify for NDIS support.
National Disability Insurance Agency (NDIA)
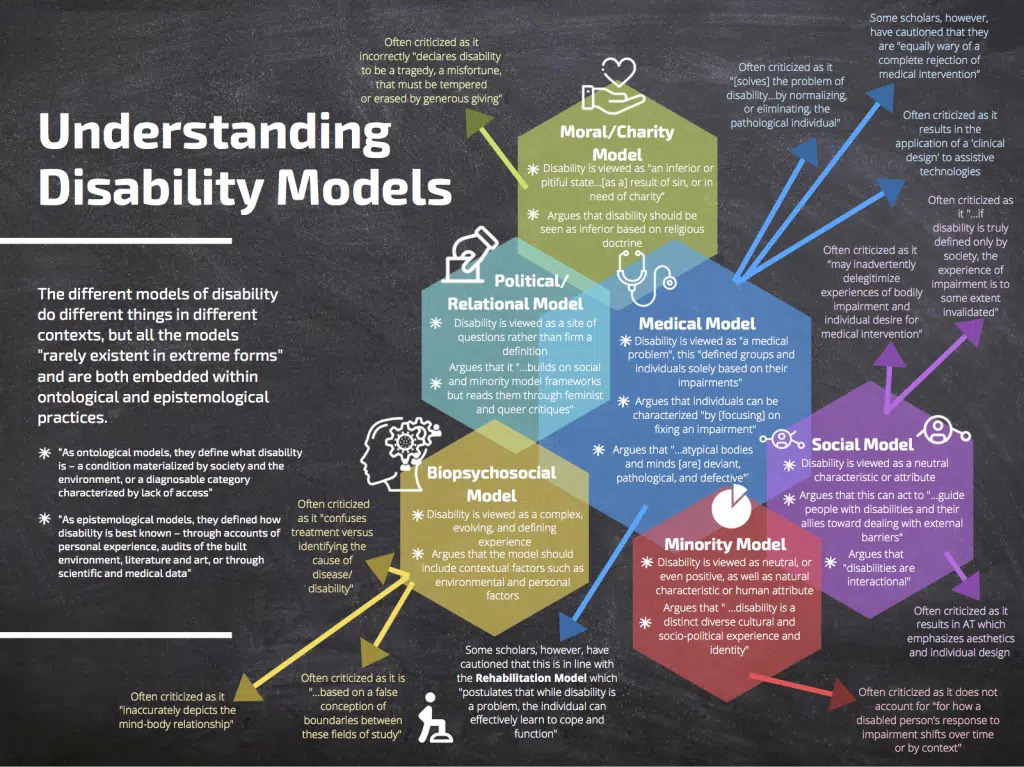
Intuited from a cursory glance at disability modelling (see appendix) and evidenced by numerous internal service reviews, independent user surveys, and stakeholder critiques(6.-18.), is the significant potential for NDIS user confusion around interpretation of the above definition for the purposes of assessing psychosocial disability and allocating ‘reasonable and necessary supports’.
For example:
It is important to note that functional capacity is a pivotal concept of the Scheme, yet obtaining consistent and meaningful assessment of functional capacity has been complicated by the absence of an explicit and measurable definition of ‘Functional Capacity’ for NDIS purposes. Confusion between the terms ‘diagnosis’, ‘impairment’ and ‘functional capacity’ has seen these used interchangeably at times. In some circumstances, this has led to severity of impairment or diagnosis being used as a measure of functional capacity(6.).
Clearly, this potential for confusion is amplified for people with an a priori disability in this domain of ‘living an ordinary life’ (i.e. people with certain intellectual/developmental disabilities(22.,26-7.,29-31.)) and unsurprising, the teleological fruits of such confusion have already been made manifest in newspaper headlines e.g.:
Psychiatrists and psychologists push to get ADHD (Attention Deficit & Hyperactivity Disorder) diagnosis on NDIS.
Sydney Morning Herald, July 7, 2023, Chrysanthos, N.
(eliciting a terse response from NDIS Minister Bill Shorten: the government has no plans to make changes to the limited list of disabilities that grant automatic eligibility for the NDIS(2.)).
Adding somewhat further to the confusion, have been recent efforts to imbue the NDIS psychosocial support ethos with a ‘recovery-oriented’ approach. Requesting that we suspend our disbelief regarding the prima facie contradiction between ‘permanency’ and ‘recovery’, proponents of ‘Holistic Psychosocial Disability Support’ (MHINDS) ask us to recognise ‘that recovery is not necessarily about cure but is about achieving a meaningful and satisfying life’.
Notably, however, some confusion has been dispelled in a related field of ‘the lived experience of disability over time’- conjecture surrounding the ‘fluctuating’, ‘episodic’, ‘cyclical’, ‘variable’ etc nature of psychosocial disablement has been accommodated in changes (‘NDIS (Becoming a Participant) Rules 2021’) which more clearly recognises that people with a permanent psychosocial disability may have impairments that vary in intensity, are episodic or fluctuating(19.).
To be both heeded and accepted with the patient forbearance typically required of users of inchoate schemes, the confusion bugbear outlined above nevertheless places it at number one in this list of:
NDIS-funded psychology- 5 things to consider:
1. ‘Don’t try this at home’

People who experience disability because of mental health issues, and are likely to be eligible for individualised NDIS support will:
- have explored treatment options as indicated by your clinician, to resolve the mental health issues (clinical recovery) and any ongoing treatment is recovery oriented; and
- be likely to need lifelong support to participate in the community and/or work.
Given that the estimated percentage of the Australian adult population in need of NDIS individually funded supports as result of disability related to psychosocial disability is expected to be 0.4 % (that is, 12% of people with severe and persistent mental illness), it may be safely inferred that the pool of experienced guides is proportionately small.
Given also the historical perspective outlined above, however, it may also be safely inferred that the NDIA has every reason to co-opt (with a bit of specialised training thrown in) the same proven cohort of stewards and gatekeepers already employed by other national insurance agency arms (i.e. Medicare), that is, (in large) Registered Medical Practitioners.
Finally, given the algorithmic nature of contemporary public resource allocation infrastructure (invariably, algorithmic tools operate to restrict access to the disability category so that fewer people can claim a political entitlement to public assistance on the grounds of disability(20.)), key signposts may be located in a small number of critical interfaces (called ‘forms’ in the old days). A good one to start with is the Evidence of Psychosocial Disability (EPD) Form.
The NDIS partners with Local Area Coordinators (LACs) who possess expertise in helping you decide whether to apply for general NDIS support or an individualised ‘NDIS package’ (i.e. an NDIS ‘Plan’); call 1800 800 110 or email enquiries@ndis.gov.au to find out which LAC covers the area in which you live.
Resource-wise, you can’t go past the NDIS Mental Health Access Snapshot Series.

“the division at the National Disability Insurance Agency where these officials now work is expanding its compliance branch using the same strategies”(31.).
2. Psychologists may only deliver non-clinical services under NDIS plans.
Don’t panic! An understanding of the difference between ‘clinical’ and ‘non-clinical’ from an NDIS perspective may be gleaned from this page.
Basically, the NDIA, through the NDIS Act, explicitly prohibits funding for services already covered by ‘universal health’ arrangements (including those currently inaccessible due to lack of reasonable adjustments required under the Disability Discrimination Act (Cth) 1992).
In the case of psychologists’ services, mental health treatment in the private and public sectors is already funded via the ‘Better Access To Mental Health Care’ (Medicare) initiative and private health insurance providers.
Interpreting the NDIS,
We don’t fund psychology as therapy or clinical treatment to address symptoms of your mental health condition. If your treatment is to stabilise or manage your mental illness, or to set up longer-term recovery pathways, the health or mental health system is responsible. We don’t fund clinical mental health treatment as a reasonable and necessary psychology support in your plan.
We may fund non-clinical supports that relate to your ongoing psychosocial disability and functional ability. This includes supports that let you do day-to-day tasks and take part in community and social and economic life,
…with some good news added for measure from the (overarching) DSS(21.);
(funding) may also include provision of family and carer supports to support them in their carer role, and family therapy, as they may facilitate the person’s ability to participate in the community and in social and economic life,
…has led to various sources speculatively proposing examples of such ‘acceptable’ psychologist-delivered psychosocial disability supports, including:
- Individual social skills training, psychoeducation, and social anxiety coaching
- Social skill performance
- Specific social competencies including theory of mind, emotion perception, and social perception
- Problem solving and coping skills
- Illness management and awareness
- Individual or group-based Cognitive Behavioural Therapy interventions focused on behaviour activation, social interactions, and social anxiety
- Cognitive reframing and remediation interventions and psychosocial disability-targeted cognitive strategies to analyse social situations and interactions
- Cognitive Enhancement Therapy and meta-cognitive training
- Behaviour activation interventions to assess, prioritise and practice individual values and goals
- Relationship-focused skills, knowledge, and behaviour training
- Sex, relationship and family planning
- Relationship abuse prevention interventions
- Life skills training interventions
- Parenting skill, knowledge, and confidence training programs
- Life Story dialectical therapy
- Art and music participation
- Psychoeducation and ehealth or SMS-based supports
- Behaviour activation interventions and other ‘non-talking’ therapeutic approaches including eye movement desensitisation and reprocessing (EMDR) modified for people with certain intellectual disabilities.
3. Does NDIS-registration matter?
Although participants whose plans are ‘Agency (NDIA) Funded’ are required to use NDIS-registered psychologists, this rationale is neither well elucidated nor evidenced in participant surveys:
For allied health workers, a sense of safety came from the fact that workers typically hold registration or accreditation with their appropriate professional bodies. Participants did not see what NDIS registration could add to their professional standards(14.).
Kim: I would see it as a dignity of risk thing. Like, I’d prefer to choose who’s in my life than have the people that the police checks deem are safe pushed it on me.
Indeed, whilst this article appears under the banner of a registered NDIS provider, there is widespread anecdotal evidence that many participants are drawn toward unregistered providers for reasons of individual innovation, desired skillset, and service accessibility, or due to ‘corporate’ aversion:
Jill: …a lot of these big companies that are NDIS registered providers, they really are based on profit, and a lot of them- for example the [occupational therapy] company, they then try and refer you to their speechies, or their physios—they’re trying to upsell.
On the other hand, professional registration does matter: providers of psychological services who are registered with the Australian Health Practitioner Regulation Authority (AHPRA) are bound by rigorous standards of training and continuing education, professional and ethical conduct, and privacy and confidentiality rules.
4. Do Service Agreements with psychologists affect the ‘therapeutic alliance’ ?
In short, no. Establishing and reviewing a service agreement (as recommended but not mandated by the NDIA for therapeutic supports delivered by a psychologist) involves the release to plan managers and support coordinators (or individuals with self-managed plans) of ‘budgetary’ information only, and has no bearing on the client-practitioner relationship.
5. What about additional mental health burdens like alcohol/drug use disorders?
Treatment for mental health conditions which may be relatable to an existing psychosocial disability meeting the requirements for NDIS funding can still only be funded by ‘traditional’ (eg using Medicare/Private Health Insurance) means, although a potential participant may be accessing, or planning to access treatment, for co-existing substance dependency at the time of access and throughout any ongoing relationship with the NDIS.
Conclusion
While the NDIS psychosocial disability pathway and Psychosocial Disability Recovery Framework were introduced to facilitate access for eligible participants with psychosocial disability, it is too early to say whether this will improve utilisation and outcomes(12.).
This article was written for educational purposes and in no way reflects the views of Brisbane Counselling Centre (a registered NDIS provider organisation). If you or someone you know are seeking an NDIS-registered psychologist, or want more information regarding ‘psychologists and the NDIS’, please feel free to contact us.
Appendix: Disability models
References
1. Edwards, T. (2019). A disabling ideology: challenging the neoliberal co-optation of independent living under the NDIS. Journal of Australian Political Economy, 83, 32–59.
2. Chris Horsell (2020): Problematising Disability: A Critical Policy Analysis of the Australian National Disability Insurance Scheme, Australian Social Work, DOI: 10.1080/0312407X.2020.1784969.
3. Gooding, P.,West, A. (2023).Disability assessments and the algorithmic veil: lessons from the abandoned ‘independent assessments’ proposal for the National Disability Insurance Scheme. Australian Journal of Human Rights, Vol 28, No. 2-3.
4. NDIS. (2020). Independent Assessment- Framework.
5. Mental Health Australia. (2019). Health professionals, psychosocial disability, and NDIS access. Final Report, Funded by the Australian Government Department of Social Services.
6. NDIS (2020). Independent Assessment- Selection of Assessment Tools.
7. National Disability Insurance Agency. (2020). Participant outcomes. To 30 June 2022
8. McKenzie, K., Smith-Merry, J. (2023). Responding to Complexity in the Context of the National Disability Insurance Scheme. Social Policy & Society 22:1, 139–154.
9. Wilson, E., Campain, R., Pollock, S., Brophy, L. and Stratford, A. (2022). Exploring the personal, programmatic and market barriers to choice in the NDIS for people with psychosocial disability. Australian Journal of Social Issues, 57, 1, 164–84.
10. Gilchrist, D., Perks, B. (2022). See no Evil, Hear no Evil, Speak no Evil: The grey literature and Australia’s failure to address change in the National Disability Insurance Scheme. Aust J Soc Issues. 2023;00:1–18.
11. Shelby-James, T. (2023). National disability insurance scheme access: What evidence do you need to provide for psychosocial disability? Australasian Psychiatry 2023, Vol. 31(2) 174–177.
12. Devine, A., et al. (2022). ‘Nearly gave up on it to be honest’: Utilisation of individualised budgets by people with psychosocial disability within Australia’s National Disability Insurance Scheme. Soc Policy Adm. 2022;56:1056–1073.
13. Green, C., et al. (2022). Market shaping: Understanding the role of non-government actors in social care quasi-market stewardship. Soc Policy Adm. 2022;56:1138–1155.
14. Yates, S., Dickinson, H., West, R. (2022). ‘I’ve probably risk assessed this myself’: Choice, control and participant co-regulation in a disability individualised funding scheme. Soc Policy Adm. 2023;1–17.
15. Boschen, K., Phelan, C., Lawn, S. (2022). NDIS Participants with Psychosocial Disabilities and Life-Limiting Diagnoses: A Scoping Review. Int. J. Environ. Res. Public Health 2022, 19, 10144.
16. Mellifont, D., et al. (2022). Barriers to applying to the NDIS for Australians with psychosocial disability: A scoping review. Aust J Soc Issues. 2023;58:262–278.
17. Winkler, D., Brown, M., D’Cruz, K., Oliver, S., Mulherin, P. (2022). Getting the NDIS back on track: A survey of people with disability. Summer Foundation.
18. Bould,E., Sloan, S., Callaway, L. (2022). Behaviour support for people with acquired brain injury within the National Disability Insurance Scheme: an Australian survey of the provider market. Brain Impairment (2022), 1–15.
19. Australian Psychological Society. (2021). Response to the Australian Government proposed NDIS legislative improvements and the Participant Service Guarantee. Submission.
20. Van Toorn, G. (2022). Towards a Social-Relational Model of Digital Disability Classification. Data and society Research Institute. https://points.datasociety.net/toward-a-social-relational-model-of-digital-disability-classification-9a0a04ebdd10.
21. PRINCIPLES TO DETERMINE THE RESPONSIBILITIES OF THE NDIS AND OTHER SERVICE SYSTEMS https://www.dss.gov.au/sites/default/files/documents/09_2021/ndis-principles-determine-responsibilities-ndis-and-other-service-1.pdf
22. Devine, D. (2018). Can cognitive behavioural therapy (CBT) work for those with learning disabilities? Learning Disability Today (15th October), https://www.learningdisabilitytoday.co.uk/can-cognitive-behaviouraltherapy-cbt-work-for-those-with-learning-disabilities.
23. Ocay, D.D., et al. (2022). Psychosocial and psychophysical assessment in paediatric patients and young adults with chronic back pain: A cluster analysis. Eur J Pain. 2022; 26:855–872.
24. Hassiotis, A. (2021). Behaviours that challenge in Adults with Intellectual Disability; Overview of Assessment and Management. Report: Camden and Islington Foundation NHS Trust and Camden Learning Disability Service.
25. Hemmings, C., Barber, L. (2018). Here’s how to support the mental health of people with learning disabilities. Learning Disability Today, https://www.learningdisabilitytoday.co.uk/supporting-the-mental-health-of-people-with-learning-disabilities.
26. Bourne, J. (2021). A systematic review of community psychosocial group interventions for adults with intellectual disabilities and mental health conditions. J Appl Res Intellect Disabil. 2021;1–21.
27. Fullerton, M. (2018). Choice making with multiple learning disabilities. Learning Disability Today. https://www.learningdisabilitytoday.co.uk/choice-making-with-multiple-learning-disabilities.
28. Nouwens, P., et al. (2017). Identifying classes of persons with mild intellectual disability or borderline intellectual functioning: A latent class analysis. BMC Psychiatry, 17, 257. https://doi.org/10.1186/s12888-017-1426-8
29. Bouvet, C., & Coulet, A. (2016). Relaxation therapy and anxiety, self-esteem, and emotional regulation among adults with intellectual disabilities: A randomized controlled trial. Journal of Intellectual Disabilities, 20(3), 228–240. https://doi.org/10.1177/1744629515605942
30. Giummarra, M.J., Randjelovic, I., and O’Brien, L. (2022) Interventions for social and community participation for adults with intellectual disability, psychosocial disability or on the autism spectrum: An umbrella systematic review. Front. Rehabilit. Sci. 3:935473.
31. Morton, R. (2022). Robo-debt ‘insights’ to shape NDIS compliance. The Saturday Paper, Nov 26 – Dec 2, 2022, No. 427.
